
.jpg "Daniel Godla")
What is Principal Care Management?
Principal Care Management (PCM) is a preventive program that helps patients mitigate one, specific chronic condition. Covered by Medicare Part B, providers should learn what CPT billing codes are used for PCM in order to optimize care delivery and avoid denied claims.
PCM is covered for Medicare Part B patients with a small co-pay. This monthly engagement program offers patients the benefits of personalized care plans and assisted development of self-management behaviors.
PCM is reimbursable under Medicare’s Physician Fee Schedule, paying various rates.
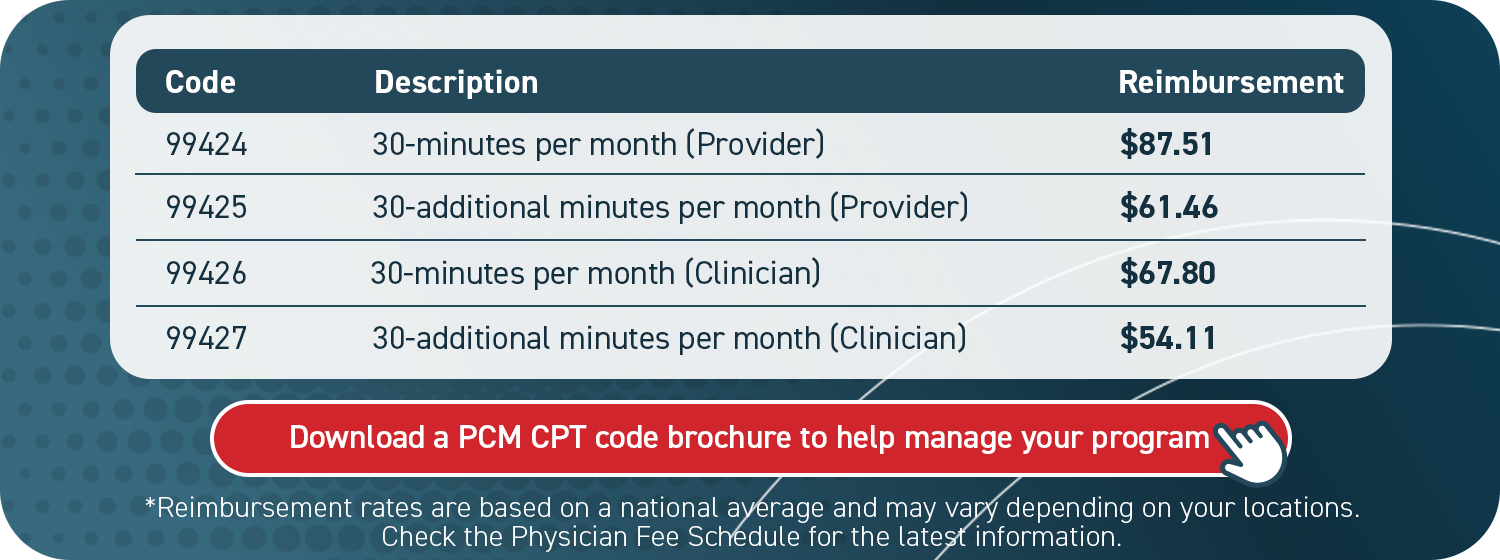
Principal Care Management CPT codes:
99424, 99425, 99426 and 99427
Different CPT billing codes reflect specific categories of PCM. The crucial qualifying determinants are who provides program services and the length of time spent with the patient.
As shown, one set of codes (99424 and 99425) is designated for providers’ utilization in 30 and 60-minute increments. The other set of codes (99426 and 99427) is for clinical staff usage also in 30 and 60-minute increments of service.
Although there may not be any difference in the services delivered between the provider and clinician code, it is important to note that utilizing the most appropriate code for who delivered the services is considered best practice in case of an audit by Medicare.
The determination between utilizing provider or clinician CPT codes would hinge on patient case complexity and provider discretion.
It is important to note that a provider cannot offer both PCM and Chronic Care Management services to the same patient in a given month. However, the patient may receive PCM services from one provider and Chronic Care Management from another as long as different conditions are being managed in both of the programs.
Medicare Principal Care Management requirements
Providers can use PCM to engage patients on a monthly basis between regular appointments.
Delivered through remote interactions, either by phone or a telehealth platform, PCM is billable when at least 30 minutes are spent with the patient performing appropriate tasks.
PCM services can include:
- A monthly clinical review
- Telephone calls
- Physician reviews
- Referrals
- Prescription refills
- Chart reviews
- Scheduling appointments or services
Eligible patients have one chronic condition expected to last at least 3 months. PCM can only be used to target this single illness. It must pose a significant risk of death, acute decompensation, or functional decline.
Individual care plans are created for, and in collaboration with, the patient upon PCM enrollment. These care plans act as a comprehensive guide to the patient’s goals, health history, and behavior.
Medicare Part B covers 80% of this benefit for patients.
Who can provide Principal Care Management?
PCM billing must be directed by a provider with an NPI number. However, clinical staff can administer most of the program, saving physician time and involvement. Eligible providers include:
- Physicians
- Physician assistants
- Nurse practitioners
- Certified nurse midwives
- Clinical nurse specialists
- Pharmacists
Submitting claims to Medicare
Five items are required when submitting a Medicare claim:
- CPT codes for each program you are managing for the patient
- ICD-10 codes tied to each of the conditions you are managing within that program
- Date of service
- Place of service (most often in-office or telehealth)
- National Provider Identifier (NPI) number
It is helpful to know the staff care coordinator assigned to a patient in case of an audit.
Four steps to bill for PCM
- Verify CMS requirements were met for each patient each month
- Submit claims to CMS monthly
- Send an invoice to patients receiving monthly PCM services
- Determine there are no conflicting codes that have been billed
Rural Health Clinics and Federally Qualified Health Centers can use individual CPT codes
CMS states in its CY 2025 Final Rule: “We believe the non-face-to-face time required to coordinate care is not captured in the RHC AIR or the FQHC PPS payment, particularly for the rural and/or low-income populations served by RHCs and FQHCs.”
Giving RHCs/FQHCs access to individual billing codes aims to improve payment accuracy. It also hopes to provide clarity about which services beneficiaries receive.
PCM with Remote Patient Monitoring
Providers can offer PCM alongside Remote Patient Monitoring (RPM).
Using digital devices, such as a blood glucose monitor, patients can capture their data and use it to inform condition management.
RPM supports its own CPT billing codes, and these can be billed concurrently with PCM, supporting dual reimbursements. However, all RPM service and time requirements must be met separately from PCM.
This is also the case for rural health clinics and federally qualified health centers. These groups must use HCPCS code G0511, though.
Learn more about RPM billing codes here.
PCM with Behavioral Health Integration
Providers can also pair PCM with Behavioral Health Integration (BHI).
BHI is a monthly care management program that helps Medicare beneficiaries address mental health concerns. When offered with PCM, integrated behavioral health supports a collaborative care model that can improve outcomes and reduce cost.
BHI supports its own CPT billing code that can be billed concurrently with PCM. However, all BHI service and time requirements must be met separately from PCM.
This is also the case for rural health clinics and federally qualified health centers when using HCPCS code G0511. Learn more about BHI billing codes here.
Revenue potential of Principal Care Management
For healthcare organizations, care management programs can drive revenue and support cost savings. Below is a general example of how reimbursement for a PCM program could add up.
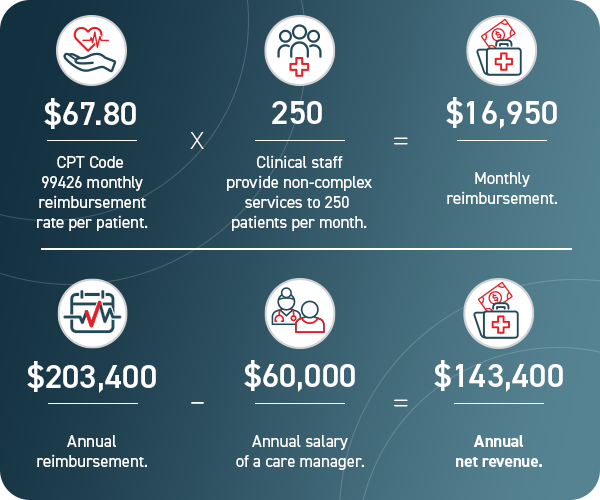
The final figure in the graphic does not account for complex or physician-driven PCM services, nor does it include additional billable time beyond the 30-minute minimum. Both could produce a higher figure.
Principal Care Management promotes value-based care
PCM programs offer additional provider benefits, beyond direct reimbursement. They can be optimized to report data, engage and motivate patients, and meet specific quality metrics key to value-based care.
PCM can enhance patient engagement and improve care coordination. Personalized care planning can be used to establish and track SMART goals, or identify social determinants of health.
Patients benefit from enhanced engagement, as well as access to a care manager. They have a monthly check-in to ask questions, discuss their condition, and access resources.
A PCM program can generate significant revenue just by billing certain CPT codes. However, elements of the program, especially within a larger healthcare system, can also promote a value-based care model.
ThoroughCare simplifies Principal Care Management
ThoroughCare gives providers the tools and support to make Principal Care Management effective.
We help providers, based on their specific needs, build PCM programs or scale existing services. ThoroughCare supports a comprehensive software platform, clinical advisement to optimize workflows and reporting tools for quality improvement.
We simplify the process, so providers can focus on engaging patients. ThoroughCare offers:
- Comprehensive care planning tools
- Evidence-based assessments (lifestyle, health risks, behavioral conditions, SDOH)
- Automated billing code assignment with audit trail
- Data integration across EHRs, HIEs, remote devices and advance care plans
- Analytics to report on care performance and operations

*Reimbursement rates are based on a national average and may vary depending on your location.
Check the Physician Fee Schedule for the latest information.