Search for topics or resources
Enter your search below and hit enter or click the search icon.
CCM is a Medicare Part-B program for patients with two or more chronic conditions. Clinical staff engage patients for at least 20 minutes per month to coordinate care activities.
Studies have shown that CCM programs can reduce hospital admissions and cut health costs in the long term. Providers are also reimbursed per patient for offering the service.

Common conditions include but are not limited to:

Facing limited clinical resources and rural health barriers, 2-G Consulting, a care management service provider, uses Chronic Care Management to close the healthcare divide.
With its care management programs, 2-G Consulting has:
Achieved an average patient retention of 23.4 months.
Boosted successful patient engagement by 36%.

CCM billing must be directed by a provider with an NPI number. That said, a diverse set of licenses can deliver the program, including:

Enrollment is completed at an in-person evaluation or Annual Wellness Visit. Written or oral consent must be documented.
The provider should explain to the patient:


Different CPT billing codes reflect specific categories of CCM. The qualifying determinants are who provides program services, complexity of medical decision-making, and the length of time spent with the patient.
Billing code assignment is based on the complexity of medical decision-making.
As shown in the graphic above, CCM billing codes specify Complex and Non-complex chronic care services. Within these categories, codes further reflect different lengths of time spent with patients and the level of physician involvement required.
In some instances, Non-complex CCM can be provided by clinical staff.
For Non-complex CCM, the following CPT codes can be used to account for reimbursement based on all program requirements being fulfilled.
Two ICD-10s must be presented when billing for chronic care services as the requirement for CCM includes two or more present conditions.
The following codes are designed for non-complex chronic care in which the provider or non-physician practitioner (NPP) is heavily involved. They cannot be billed concurrently with standard CCM CPT codes (reviewed in the prior section).
The value of physicians’ time is reflected in these non-complex, physician-driven codes as CCM services are not reliant on clinical staff:
The following billing codes apply for complex care:
It is important to note the distinction between CPT code 99487, which accounts for 60 minutes of complex chronic care, versus the two CPT codes (99491 and 99437) that account for 60 minutes of physician-driven, non-complex chronic care.
In the case of a Medicare audit, you will want to show the correct code was applied based on the compatible situation.

Apart from understanding CCM's rules and requirements, providers should:

Organize a multidisciplinary team of qualified providers to support a comprehensive CCM program, and determine appropriate roles and responsibilities.

Find eligible CCM patients by targeting specific conditions or populations, working with specialists and primary care partners, or reviewing current EHR records.

Acquire a digital platform to streamline workflow, support documentation, enable patient care planning, track and report outcomes, and automate claims preparation.
CCM can be a versatile tool to maximize care quality and performance.
Though it's a fee-for-service program, CCM can help providers address value-based care objectives without sacrificing financial stability.

Care gap closure isn’t about checking a box.
CCM programs can help patients understand the value of prevention throughout every phase of life.
Goal-oriented care engages patients in identifying their personal objectives and aligning their care with these desired outcomes.

Payors and providers can use CCM to save more than $800 per case, reducing readmission and inpatient days, as well as lowering post-acute utilization rates.

Since 2017, ThoroughCare has helped MetaPhy Health optimize care delivery for patients with multiple chronic conditions.
Learn how MetaPhy Health uses our care coordination platform.

CCM programs can directly influence and support quality improvement efforts, leading to better health outcomes and performance measures, as well as value- or performance-related financial incentives. For rural communities, a CCM program can capitalize on providers’ strengths in nurturing personal relationships and maximizing limited resources.
They can leverage close ties to the community and collaborate toward quality improvement efforts.

A Chronic Care Management program in West Virginia was so successful that it was scaled to three states, including 11 Federally Qualified Health Centers and three rural hospitals. This program leveraged community health workers to support patients living with diabetes and achieved improved health, including:

Studies highlight specific ways CCM enhances care quality, including:

This can further support patient outcomes and generate additional reimbursement.
Patients can use digital devices to capture health data for more informed chronic care.
Providers can help address behavioral health as part of overall care for chronic illness.
.png?width=110&height=110&name=ThoroughCare%20Icon_TCM%20(1).png)
Patients can receive support following a hospital discharge to avoid readmission.
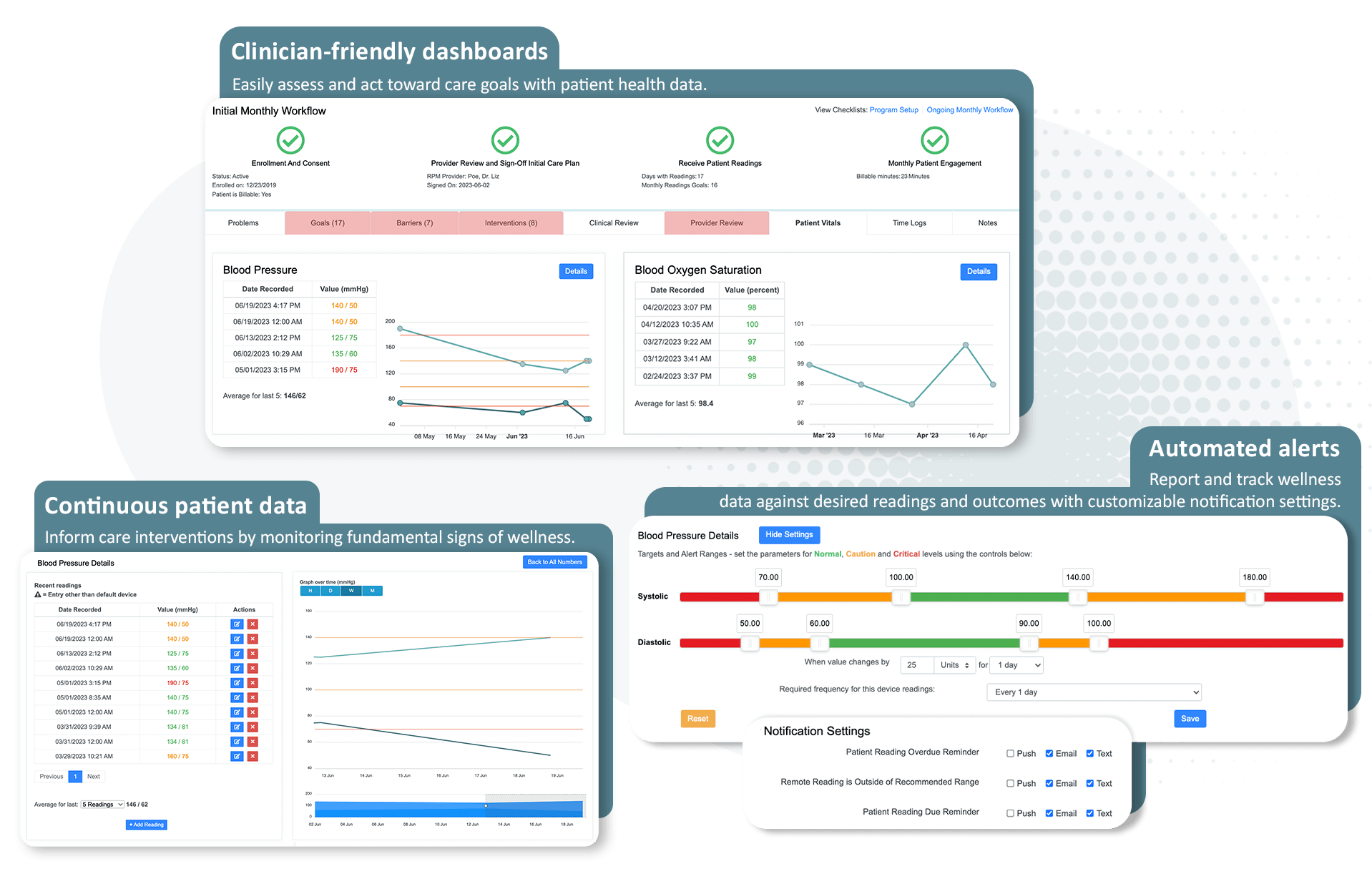
Remote Patient Monitoring encourages patients to collect and watch their physiological vitals. Providers can use this data to inform chronic condition management.
The dashboards shown are from ThoroughCare's care management software platform.
One of the powerful aspects of Medicare care management programs is that some are designed to work together.
CCM and RPM can be billed together when each program independently meets the requirements set by the Centers for Medicare & Medicaid Services.


ThoroughCare gives providers the tools and support to make Chronic Care Management effective.
We help build programs or scale existing services.
ThoroughCare supports a comprehensive software platform, clinical expertise to optimize workflows and assistance with data and reporting for quality improvement.
