

What You'll Learn Reading This Article
- Patient-Centered Care Plan Definition: A patient-centered care plan is a collaborative, living document owned by the patient and shared across the care team to tailor treatments, goals, and interventions to an individual’s unique physical, emotional, and social needs.
- Clinical and Financial Benefits: Implementing individualized care planning improves patient satisfaction, enhances medication adherence, reduces fragmented care, and actively mitigates billions of dollars in wasted healthcare spending caused by poor care coordination.
- Value-Based Care Alignment: Ongoing care management programs—such as Medicare’s Chronic Care Management (CCM)—leverage patient-centered planning to streamline clinical workflows, hit value-based metrics, and drive recurring fee-for-service reimbursement.
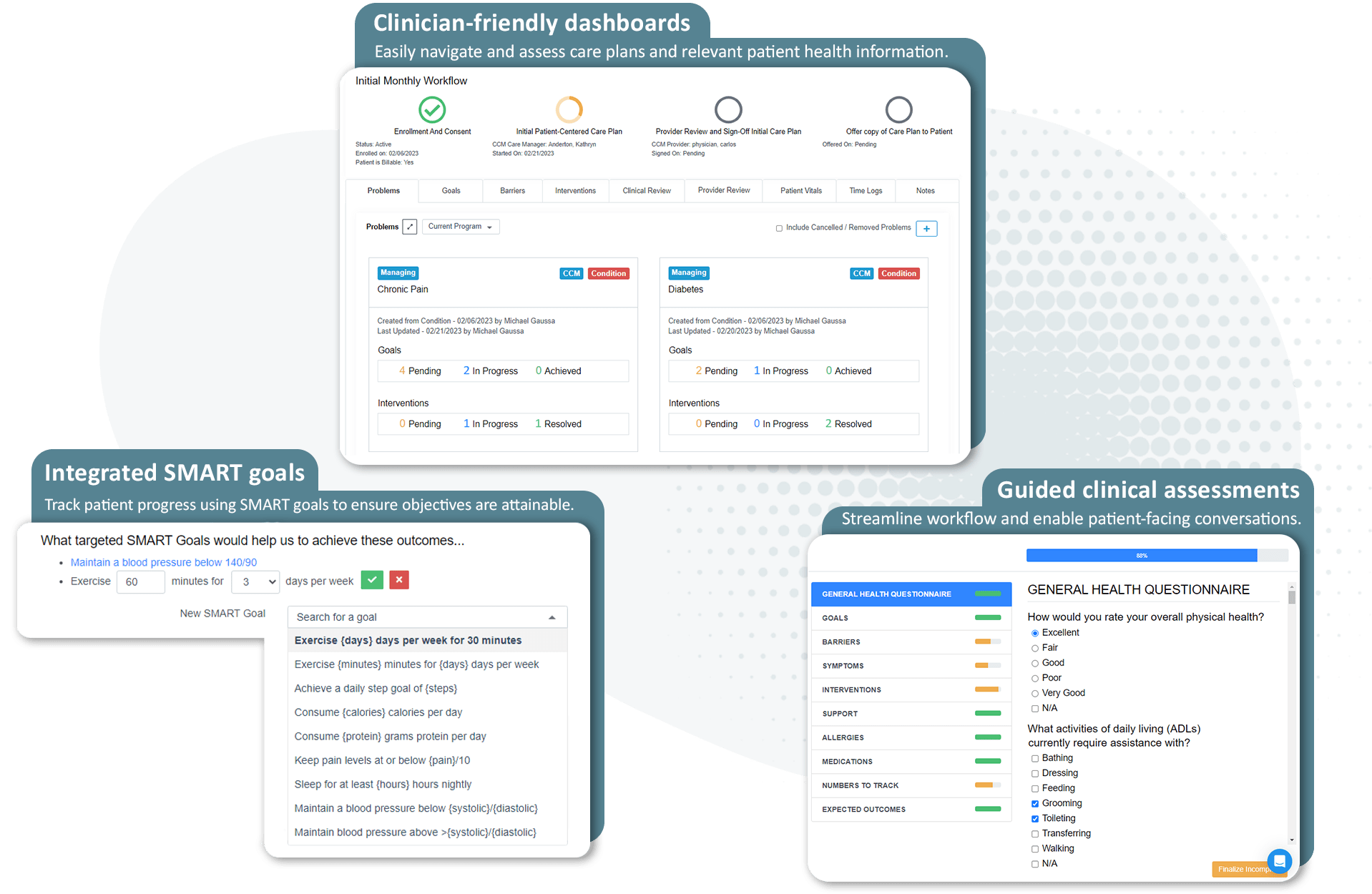
- The ThoroughCare Solution: As a comprehensive care coordination platform, ThoroughCare enables clinical teams to seamlessly build these evidence-based, patient-centered care plans through guided workflows, risk factor analysis, and CMS-compliant tracking.
Many physicians and clinicians pride themselves on the relationships they develop with their patients. By creating a patient-centered care plan, providers can enhance engagement, deliver timely interventions, align on outcome goals, and improve care team coordination.
At broadest, a care plan is a living document that captures a patient’s current health information and conditions. It outlines treatments, care services, and goals the provider will help patients receive or address.
A patient-centered care plan considers the beneficiary's individual needs, and it is created in collaboration with them. The patient is the owner of this document, but it can be shared between care team stakeholders, as well as family members, based on their consent.
A patient-centered care plan differs from a standardized one, since the standardized one is already pre-developed to specific conditions and is not tailored to the beneficiary's exact needs. Clinical teams, including nurses or care managers, can use the patient’s individualized plan of care to coordinate activities and services. This can help prevent duplicative efforts, promote patient data sharing, and potentially cut costs.
Care planning can involve ongoing conversations and engagement with patients, beyond the initial plan development. Once a care plan is created, whether for general coordination of services or a specific program, it is revisited regularly to:
- Ensure interventions and services align to patient goals and desired outcomes
- All current and accurate health information is captured
- Updates are made based on condition needs or ongoing management
As chronic disease management, value-based care, and integrated behavioral health become more of a focus for primary care, ensuring that all services are patient-oriented and can support better outcomes and improve patient and provider satisfaction.
Common features of patient-centered care plans
Though each patient-centered plan of care is unique to the individual, all should support the following:
1. Collaboration and coordination
The care a patient receives is most effective when it is collaborative, coordinated, and accessible. When implemented at scale for a chronic disease population, practices can see improvements in both outcomes and cost effectiveness. For instance, a study published by the Journal of the American Medical Association (JAMA) found that the inability to coordinate care effectively accounts for $29.6 billion to $38.2 billion in wasted healthcare spending per year.
The Financial Impact: Lowering Total Cost of Care
While historical data has long suggested the value of care coordination, real-world data (see this study published in medRxiv: Cost Impact of Chronic Care Management Services in a Large Multi-Specialty Practice) quantifies the macroeconomic impact of structured care planning at scale.
According to the multi-specialty study, Medicare beneficiaries actively enrolled in a CCM program demonstrated a 17.1% reduction in total adjusted healthcare costs compared to non-enrolled peers. This shift is driven entirely by proactive acuity mitigation. This is due to the fact that dedicated care managers track minor symptom changes early, and the study documented a 66.7% drop in inpatient hospital admissions and a 64.6% reduction in hospital-based clinic visits. For healthcare networks transitioning to value-based care, these metrics prove that individualized care plans are an essential mechanism for reducing emergency department utilization and avoiding costly 30-day readmission penalties.
An individual care plan should focus on making the patient journey seamless. It should support clinicians in aligning front-line patient care, clinical care, and ancillary and support services. This is crucial to:
- Reduce fragmentation or duplication of services and tests
- Improve patient satisfaction and engagement
- Enable more holistic, person-centric care to improve outcomes
To create an effective care plan that reflects these priorities, providers should tap into their relationship with patients to become partners. Active collaboration and shared decision-making among patients, families, and providers is key.
Specially, with patients, making them feel part of a collaborative process is important to help motivate self-care and management, as well as enable measurable progress on specific goals.
2. Physical and emotional care
Under the patient-centered care model, both physical and emotional care is provided. Physical care is provided through pain management, assistance with activities and daily living needs, and even the environment in which the care is provided.
Care plans can bolster these efforts by:
- Accounting for current medications or interventions and implementing others
- Educating patients about their specific conditions and how best to live with them
- Supporting behavioral and lifestyle changes through proactive goal setting
- Assessing social determinants of health (SDOH) to identify barriers to care and potential needs for community support or other resources
Emotional care can help treat a patient’s anxiety in dealing with chronic illnesses, physical limitations and treatment effects, as well as its impact on their family and lifestyle.
Results from evidence-based assessments, such as PHQ-9 (Depression), GAD-7 (Anxiety), or MDQ (Mood Disorders), can help patients and clinicians further tailor care plans for emotional needs, or identify gaps in care.
3. Involvement of informal caregivers and community supports
Home and community-based family and friends are an essential part of the patient-centered care model.
Including them in the patient’s care and planning adds another layer of support both physically and emotionally while also giving physicians an advocate in the home.
Providers can involve additional stakeholders by:
- Including the patient’s family or support network in all care discussions. They can help the patient understand concerns or know what their health plan offers, or provide caregivers with additional medical history.
- Educating family members or supporting individuals alongside the patient. They may also be unfamiliar with specific health effects from conditions or how certain medications work.
- Considering the patient’s values. Speak to family members and approach goal setting with your full understanding of the patient. Also consider possible language barriers, health literacy issues, and other SDOH factors.
Often, a family member or friend can help motivate, educate, and engage the patient, as well as ease patient concerns.
Care plans that are created through a digital platform can often be easily shared with key stakeholders, promoting greater accessibility.
4. Continuity in treatment
Care management programs facilitate ongoing monitoring, education, and intervention. Care can continue through regular touchpoints between in-person visits, supporting the patient’s progress, care plan adherence and lifestyle choices.
One example is Chronic Care Management (CCM). A Medicare Part-B program for patients with two or more chronic conditions, clinical staff can use this service to engage patients for at least 20 minutes per month and coordinate care activities.
Studies have shown that CCM programs can reduce hospital admissions and cut health costs in the long term.
Along with supporting care plan use for patients, a Chronic Care Management program also includes:
- A monthly clinical review
- Telephone check-ins
- Physician reviews
- Referrals
- Prescription refills
- Chart reviews
- Scheduling appointments or services
The Digital Evolution: Advanced Primary Care Management (APCM)
The operational model for care planning shifted fundamentally with the Centers for Medicare & Medicaid Services (CMS) introduction of Advanced Primary Care Management (APCM) codes. While traditional CCM relies heavily on strict, time-based logging (such as hitting minimum 20-minute telephonic thresholds), APCM updates care plan delivery for modern medicine.
APCM emphasizes continuous, asynchronous communication, integrating patient-facing mobile apps, secure digital messaging, and remote physiological tracking into the patient’s living care plan. This regulatory shift allows clinical staff to manage care seamlessly as conditions fluctuate, rather than waiting for a monthly phone call, making continuous care delivery significantly more scalable for primary care practices.
5. Transparency and knowledge
Physicians build positive patient relationships by being upfront and honest. That transparency helps when working with patients to manage chronic illnesses or complex clinical scenarios.
Creating a patient-centered care plan leverages that transparency when it comes to setting goals, gaining commitment to healthier behaviors, and educating patients on self-management techniques. Not only does this enhance quality and safety performance but it builds patient confidence in managing their own health.
Standardized care plans: ThoroughCare helps providers engage patients in evidence-based care planning
ThoroughCare is a comprehensive platform that helps providers streamline care coordination and management.
What Prevents Patient Enrollment in Care Management?
Despite the proven clinical and financial advantages of structured care planning, many healthcare organizations struggle with low patient enrollment and engagement rates. Recognizing these institutional and patient-facing friction points is the first step toward scaling an effective care coordination program.
The primary barrier to care plan enrollment is Lack of Trust & Understanding. Patients are not always educated on the meaning of care planning & coordination, and they can be led to believe there are hidden costs. This may lead patients to not understand the potential benefits of care planning, signifying the importance of clarity when involving patients in their care planning.
How a plan of care benefits patients
Beyond the trust developed with a physician and their care team, a patient-centered care model offers many benefits to patients that also, ultimately, benefit healthcare providers.
1. Improved experience and satisfaction
Providing a beneficial patient experience is its own goal. However, according to the Agency for Healthcare Research and Quality, “substantial evidence points to a positive association between various aspects of patient experience, such as good communication between providers and patients, and several important healthcare processes and outcomes.”
These can include:
- Improved patient safety practices
- Less use of unnecessary services
- Adherence to medical advice
Involving patients in the decision-making process of their care also makes them feel valued and empowered. A patient-centered care plan puts the patient in the driver’s seat as it addresses their individual needs, preferences, and unique values.
By taking a collaborative approach to the patient’s healthcare and respecting their needs, their overall experience is improved and satisfaction scores tend to respond.
2. Proactive, collaborative engagement
Within primary care, the patient-centered care model aims to fully inform someone about their health. This includes the full scope of their conditions, their prognosis, and the actions patients and providers can take to improve care.
Any success depends, however, on engaging patients in effective, measurable ways that improve outcomes. The plan of care can serve as a recurring touchpoint to connect the patient with their care manager or nurse.
Through these regular meetings, a clinician can use health information captured within the care plan to personalize engagement and monitor progress on certain outcomes. Care plans can also leverage motivational interviewing techniques to help patients act toward greater self-management.
3. A focus on better health outcomes
Preventive healthcare is generally considered an effective way to identify health risks earlier. This can help providers address certain conditions before they cause others.
Patient-centered care plans facilitate a regimen of standard preventive care services, including screenings, vaccines, and medication review. This can also have a positive impact on any present conditions.
According to the British Journal of General Practice, care planning has been shown to “improve patients’ confidence and skills in self-management. There is evidence that among engaged patients it can improve health outcomes.”
How a patient-centered care plan benefits providers
While a patient-centered care model focuses on improving an individual’s health outcomes, the benefits afforded to the physician and the larger care organization are numerous.
1. Improved patient satisfaction
By improving your patient’s health and experience, your practice will see improved satisfaction scores among patients and their families.
These scores can boost the practice’s reputation, supporting loyalty and word-of-mouth that leads to growth and revenue.
Patient experience surveys, such as the Consumer Assessment of Healthcare Providers & Systems (CAHPS), account for standardized measures related to satisfaction. They can also impact provider payment under specific value-based care contracts.
Data from the 2025 Person-Centered Primary Care Measure (PCPCM) Survey underscores exactly how comprehensive care planning impacts these quality scores. Standardized evaluations reveal that when a provider's workflow ensures a patient feels their "entire health history and life circumstances are considered" (the very definition of a patient-centered care plan), overall practice experience ratings consistently surge well past national averages, hitting 82% to 86% positive sentiment. For providers tied to value-based care contracts, this optimization directly influences performance metrics and bonus payouts.
2. Greater care team experience and loyalty
One of the biggest reasons people choose to work in the healthcare industry is that they want to help people. The relationships between staff and patients are at the core of the patient-centered care model.
As a practice provides improved quality of care and realizes higher levels of patient satisfaction, the employee experience improves as well. A happier, more engaged care team supports greater productivity and quality performance, while mitigating the risk of burnout.
3. Increased revenue and growth
While many benefits may be intangible or downstream, practices can see an impact on their bottom line through:
- Increased efficiencies
- Improved resource allocations
- New revenue streams
- New opportunities from value-based care contracting
Care management programs that rely on care planning also support fee-for-service reimbursement. Providers can use this revenue to hire and expand care teams to address quality performance goals.
4. Alignment with value-based care objectives
As mentioned above, care planning can help improve patient satisfaction surveys. But beyond this one measure, plans of care enable a personalized approach that is key to implementing value-based care.
Delivering streamlined care management and team-based coordinated care—coupled with a patient-centered approach—helps practices become more efficient, enhance quality and care outcomes, and transition to more risk-based arrangements.
Chronic Care Management programs that utilize patient-centered planning can give providers a standard workflow to hit value-based metrics.
How to create and update a plan of care
A care plan created as part of comprehensive care management should include the following five elements:
- Systematic assessment of the patient’s medical, functional, and psychosocial needs
- System-based approaches to ensure timely receipt of all recommended preventive care services
- Medication reconciliation with review of adherence and potential interactions
- Oversight of patient self-management of medications
- Coordinating care with home- and community-based clinical service providers
Once a patient is enrolled in a care management program and medical or behavioral conditions have been identified and prioritized, it’s time to lay the foundation for improved health through collaboration, coaching, and healthy actions.
Creating a care plan involves talking to the patient and collecting personal information and health data. This process can be facilitated through questionnaires or guided interviews. Data can include:
- Medical history and personal details
- Emergency contacts
- Information specific to any existing chronic conditions and related medications
- Desired outcomes and goals
- Health plan coverage
- Broader care team information to assist with coordination of services
While there isn’t one specific way to create a care plan, there are general best practices providers can follow. These can be critical talking points that ensure the most effective plan of care is developed. These can include defining the patient’s goals, identifying barriers to achieving them, and deciding which metrics to track.
Defining SMART goals through care planning
SMART goals have been demonstrated to help patients create healthier habits. They establish clear, internally-motivating, and measurable targets that align to the person’s desired outcomes. By using the care planning process, nurses can work with patients to identify where these opportunities might be.
Care managers can also create action plans to give patients a feasible, step-by-step method to integrate their goals into daily life. Together, the patient and provider can consider the circumstances that might disrupt progress. This exercise can help develop other options for when barriers emerge.
Evidence supports the effectiveness of SMART goal-setting in healthcare.
An analysis by the U.S. Preventive Services Task Force on SMART goal efficacy found they effectively reduced weight or improved eating behavior in 65% of studies. The Journal of Pharmacy Practice found that patients who set SMART goals lowered their A1c.
Identifying gaps in care
Care managers can use the patient’s plan to review any preventive services or upcoming screenings that are due and address any care gaps. Left ignored, these gaps lead to further complications in health, such as late or missed diagnosis or comorbidities.
The Future of Care Coordination: How AI is Transforming Care Planning
Artificial intelligence (AI) and machine learning (ML) are shifting patient-centered care planning from a reactive process to a predictive, automated discipline. Instead of clinicians manually scanning charts to find gaps in care, modern AI care coordination software acts as a clinical force multiplier.
According to a 2026 healthcare automation analysis, implementing advanced clinical algorithms allows practices to realize significant operational and predictive benefits:
- Predictive Risk Stratification: Advanced AI engines analyze Electronic Health Record (EHR) data, social determinants of health (SDOH), and real-time remote patient monitoring (RPM) biometrics to predict which chronic patients are at the highest risk for acute decompensation or a 30-day hospital readmission.
- Automated Care Plan Generation: Generative AI solutions assist clinical staff by analyzing immense datasets to instantly draft evidence-based, personalized care goals and medication reconciliation alerts. This drastically reduces administrative burdens, allowing nurses to focus on direct patient engagement rather than documentation.
- Dynamic Workflow Automation: AI streamlines multi-specialty care by automatically routing tasks, such as scheduling preventive screenings or alerting a pharmacist to a potential drug-to-drug interaction, ensuring the living care plan is updated asynchronously without manual human intervention.
For modern practices, leveraging platforms that integrate AI with compliant frameworks like Chronic Care Management (CCM) and Advanced Primary Care Management (APCM) is no longer just an efficiency upgrade, it is a core strategy for scaling value-based care outcomes.
How ThoroughCare creates patient-centered care plans
The ThoroughCare platform provides evidence-based assessments, education, and workflows to enable a patient-centered care planning approach. We give nurses and care managers the tools to take all necessary steps required by CMS for care management delivery.
Featuring clinical content based on recommendations from the American Academy of Family Physicians, our guided interview walks care managers and nurses through a patient-centered care plan, providing the most common questions and answers to effectively identify, manage, and treat every patient’s chronic conditions.
Additionally, ThoroughCare can help clinicians:
- Help motivate patients through clinical recommendations
- Analyze patient risk factors and generate clinical recommendations
- Identify behavioral health conditions
- Track and log services for an audit-proof record of care
Next-Generation Automation: ThoroughCare AI
To support practices scaling their value-based care objectives without succumbing to clinical burnout, the platform features ThoroughCare AI.
This advanced system fundamentally changes how care plans are updated and maintained during patient interactions:
-
Automated Transcription and Call Summarization: When care managers conduct monthly telephone check-ins, ThoroughCare AI captures, records, and transcribes patient discussions in real time. This allows clinicians to focus purely on empathetic engagement rather than manual note-taking.
-
AI-Generated SMART Goals: The AI engine cross-references the live transcript with the patient's existing clinical history to automatically generate contextually relevant, data-driven SMART goals and task suggestions, posting them directly into the care plan.
-
Intelligent Call Guides: Care teams are equipped with dynamic, evidence-based call guides containing documented sources for all clinical insights, ensuring the highest standards of safety and compliance during chronic care delivery.
According to real-world deployment data, care teams utilizing ThoroughCare AI reported a 25% increase in operational efficiency alongside a 27% boost in patient retention. By turning unstructured conversations into actionable care plan interventions automatically, the platform provides an optimized roadmap for profitable, high-quality care coordination.
