

A transition of care (ToC) involves moving a patient from one care site to another. These “moments of truth” are critical to ensuring continuity of care that is safe, efficient, and supports a successful healthcare journey.
Care transitions can include movement between hospitals, skilled nursing facilities, and homes or between an ICU to a cardiac rehabilitation center. Other specific instances of transition are applicable, as well.
Poor transitional care management, however, can lead to significant patient safety issues and cost burdens. With more than 3.8 million hospital readmissions annually in the US and an average readmission cost of $15,200, care transitions are now a key focus for quality performance measurements and improvement.
Transitions of care are ubiquitous (and costly)
Transitions of care entail extensive discharge planning. This involves informing and equipping the patient and their family to manage self-care. For care management providers, transition support may include:
- Scheduling follow-up appointments
- Making referrals
- Arranging new treatments or equipment
- Medication management and reconciliation
- Self-management education and care plan adherence
- Community or social services
Figure 1 visualizes the eight types of transitions of care among various care settings. These ToCs can happen within one care setting, between or across locations, or among providers.
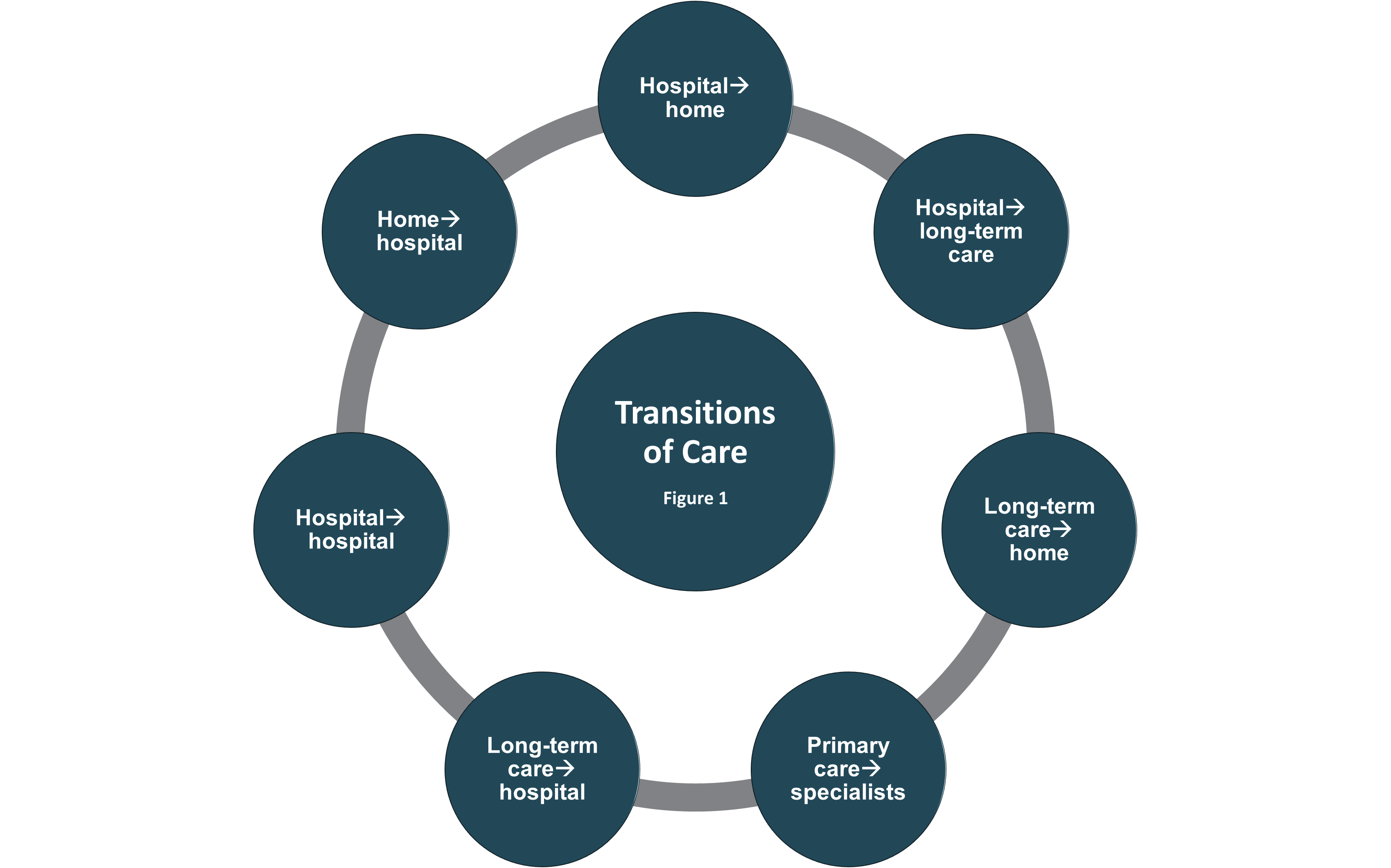
One or more of these transitions can occur within a single medical episode.
"The big risk for errors is from acute care to where the patient goes next – rehab, home or nursing home. Discharge plans are so complex now, but if they aren't followed closely, the patient will get readmitted, and now there are penalties. If you don't get the transition right and the readmission could have been avoided, it will cost the system more money." - Tom Sullivan, MD, chief strategic officer for Rockville, Maryland-based DrFirst
Readmissions from post-acute care providers to acute care environments are of specific concern to healthcare organizations, particularly because they can come with a penalty from Medicare. According to the Centers for Medicare & Medicaid Services (CMS), they amount to more than $26 billion annually and affect almost 20% of beneficiaries.
Transitional care benefits quality outcomes
The Institute for Healthcare Improvement (IHI) estimates that a comprehensive Transitional Care Management (TCM) program can help acute care providers reduce readmissions.
The objectives of an effective TCM program include:
- Care quality and patient outcomes, encompassing safety, efficacy, patient-centeredness, timeliness, efficiency, and equity
- Patient experience through provider accountability and care delivery innovation
- Provider experience through improving communication and capacity while reducing administrative burden
- Population health by preventing disease escalation
- Spending by reducing avoidable utilization and payment model innovations
A 2023 report, titled Impact of Transitional Care Management Services on Utilization, Health Outcomes, and Spending Among Medicare Beneficiaries, found that TCM patients had:
- Experienced fewer rehospitalizations
- Lower total Medicare Parts A and B spending
- Almost one-third of an additional healthy day at home
A McKinsey analysis demonstrated the value of TCM. When patients with similar risk scores were modeled, those who did not receive proper follow-up had a 23% greater likelihood of 30-day readmission.
Additionally, value-based care initiatives are incentivizing lower readmission rates when tracked by quality performance metrics. This can include appropriate length-of-stay measures and care management that supports higher-risk patients.
Creating a transitional care management program
Designing an end-to-end streamlined transitional care management program depends on five components, including:
- Data interoperability
- Predictive analytics
- Software technologies
- Workflow orchestration
- Transitional team members
Each component plays a critical role in planning, communication, coordination, and team-based care across sites. They work in tandem, providing data insights, risk stratification, and timely activity in a systematic fashion.
Data interoperability
Data interoperability is probably the most critical aspect of modern ToCs. Having accurate, accessible, and timely information and documentation is the heart of effective transitions. Interoperability ensures that the right people can exchange information seamlessly.
A 2022 survey revealed that 99% of hospitals and physicians are more likely to refer patients to post-acute providers that offer interoperability. That same study found that 72% would be willing to switch vendors who offered a system that met their most essential interoperability requirements.
Additionally, health information exchanges (HIEs) have been shown to improve care by providing health information at critical times of need.
Predictive analytics
Robust data analytics can help stratify high-risk patients and provide guidance on how to manage their transitions of care. Claims-based machine learning models are often used to generate accurate predictions for transition planning.
Real-time decision support analytics, for instance, can recommend the next best site of care for a patient. In fact, discharge destination has been shown to be a significant indicator of readmission.
Real-time decision support could provide visibility into network and claims data to show the best subsequent care destinations.
Software technologies
While 50% of surveyed hospitals and health systems only use their electronic health record (EHR), 25% are considering stand-alone platforms for transitional care management.
Care coordination platforms play a crucial role in communication across care teams. They can support continuity of care at a critical time when patients must adjust to new medications and self-care activities.
Workflow orchestration
From the time when a patient is admitted, their subsequent discharge and transition depend on workflow orchestration.
Care managers work with case managers at hospitals or skilled nursing facilities to lay the groundwork for a successful discharge. This can include:
- Creating or using the patient’s care plan
- Expected length of stay
- Types of needs after their stay
- How family caregivers and other provider team members can support the transition
Transitional team members
Several ToC models provide guidance on the number and types of roles necessary for a TCM program. These models may include:
- Transitional Care Management Framework
- Project RED (Re-Engineered Discharge)
- Project BOOST (Better Outcomes for Older Adults Through Safe Transitions)
- Explicitly defining and equipping specific care transition roles and responsibilities is foundational.
Tech-enabled integrated teams are at the crux of ToC activities. For example, Kaiser Permanente’s Northwest US branch reduced its all-cause readmission rate by nearly one-third by introducing a post-discharge team-based strategy.
A New York–based health plan reduced readmissions by 21% for its dual-eligible Medicare and Medicaid members. It did so through provider coordination, patient communication, at-home visits, family engagement, and patient education.
According to McKinsey, “tech-enabled data sharing, readmission analytics, workflow modules, and health services partnerships provide the basis for high-ROI ToC program design.”
Health plans and provider organizations are working together to prioritize the deployment of high-touch, actively-managed care transitions.
Keeping patients at the center of transitions of care
Even with the best data-sharing technologies, a stellar care team, and a well-oiled workflow, it’s pivotal that the entire care team understands the challenges patients face.
When patients are discharged from one care setting to another, they can be overwhelmed with change. New or adjusted medications, new self-care activities, and changes to health routines take time and support to be successful.
It’s critical that everyone involved provides timely, consistent, and compassionate follow-up, education, and support. This not only supports patient safety through transition, but addresses care beyond discharge that avoids costly readmissions.
How ThoroughCare can help
ThoroughCare helps deliver integrated care management services to foster patient engagement and enhance revenue. Our platform provides the digital infrastructure to leverage fee-for-service programs while promoting value-based care objectives.
ThoroughCare supports end-to-end workflow for TCM, including:
- Tracking and reporting hospital discharges
- Coordinating time-sensitive transitional care services
- Simplifying reimbursement with automated CPT code assignment and an audit-proof record of care
