

According to research published in the journal Primary Health Care Research & Development, there is strong evidence that care management benefits patients and providers by:
- Increasing patient adherence to treatment guidelines
- Improving patient satisfaction
However, how do care teams ensure patients' and organizational goals are met?
Care management was created and became reimbursable because it provides a standardized, team-based, and personalized approach to help patients with chronic conditions. Addressing these comorbidities strives to decrease a patient’s risk of experiencing gaps in care.
Critical to care management’s success, however, is understanding and targeting the unique outcomes patients want while also meeting the needs of the provider organization.
Here, we offer the patient’s perspective on care management alongside the healthcare provider’s. This, along with evidence-based strategies, can direct the program’s focus, investment, and performance.
Unlock the benefits of care management:
A common story of patients and practices
Many patient stories have a common pattern by the time they enroll in care management. Equally, there is a typical journey that leads practices to launch their own care management programs.
From the patient’s perspective: Meet Maria
The Commonwealth Fund published a case study based on an anonymous, composite patient profile.
Maria’s story highlights many objectives patients wish to realize when they understand the value and contribution that care management can give them, as shown in Figure 1.

Figure 1: Care Management provides a structure, process, and approach to achieve patient and provider goals.
Maria Viera, age 75, takes a dozen medications to treat her diabetes, high blood pressure, mild congestive heart failure, and arthritis. When she begins to have trouble remembering to take her pills, she and her husband visit her primary care physician to discuss this and a list of other worrisome developments, including hip and knee pain, dizziness, low blood sugar, and a recent fall. Maria’s primary care doctor spends as much time with her as he dares, knowing that every extra minute will put him further behind schedule. Yet, despite his efforts, there is not enough time to address her myriad ailments. She sees several specialists, but no one talks to all her providers about her care, which means she may now be dealing with conflicting recommendations for treatment, or medications that could interact harmfully. As a result, Maria is at high risk for avoidable complications and potentially preventable emergency department visits and hospital stays.
From this excerpt, the patient’s desires and those of her caregiver-husband, are clear. They are worried about the growing complexity of her clinical picture and are confused by conflicting information from different physicians. She is at risk and fearful of things getting worse or having to go to the hospital.
From the provider’s perspective
Maria’s story highlights the challenges that providers face.
Her primary care doctor wants to spend more time sorting out her complex medical situation but can’t. There is no leader of her care team to make sense of the myriad treatment protocols and medications.
If Maria is within a value-based care arrangement, her providers are at risk from avoidable exacerbations, complications, and healthcare utilization.
In addition to wanting to provide more comprehensive and value-based care to patients, healthcare providers have clear quality, safety, utilization, and revenue objectives like those listed in Figure 1.
Value both patients and providers seek
Patient-centered care prioritizes the person in all decisions, plans, and actions. Based on standardized assessments, care managers tailor the service to the individual patient, their values, personal goals, and preferences.
Through care planning, regular monitoring, and ongoing support, care managers build rapport and trust with patients. They engage and activate the patient’s participation in the care plan.
Care management programs also have a positive effect on physicians.
One study found that doctors in the intervention clinics who enrolled two percent or more of their patients in care management experienced increased productivity and were more satisfied with their profession.
The care manager’s role
Chronic conditions, such as diabetes, heart disease, and respiratory disorders, significantly impact patients’ lives, requiring a specialized approach to manage them and limit their progression. They often require continuous medical attention and can make daily activities challenging, which can lead to more severe health complications as patients age.
The care manager’s role has been studied and broken into seven activities, including:
- Initial and ongoing assessment of patients and their needs
- Facilitation, coordination, arrangement, and/or scheduling of services, supplies, treatment, and interventions
- Monitoring and following up with patients
- Education of patient and/or family
- Advocacy for patients
- Collaborative problem-solving and support
- Documentation
Chronic Care Management focuses on the patient more than their condition. This orients the care manager’s role toward helping patients live their best lives within the context of their values, preferences, and personal goals.
As an advocate for a patient’s wellness—physically, socially, and mentally—care managers listen and adapt, working to create a care plan that respects the individual's dignity and desires while being practical and sustainable for the family.
According to a case study published by the Commonwealth Fund, care managers who successfully complete training develop skills that help patients achieve their goals. These skills include:
- Empowering patients with multiple chronic conditions to organize, prioritize, and implement suggested strategies for self-management
- Identifying barriers to care and helping patients overcome or eliminate them when possible
- Coordinating resources and community referrals to connect patients with necessary and timely services
- Identifying risks to the patient’s current condition and coordinating interventions
- Gathering and interpreting data analytics to identify problems and trends
Care management strengths that meet patient and provider goals
A team from Johns Hopkins University conducted a review for the Institute of Medicine, identifying 15 models of comprehensive care for older adults with chronic illness. As highlighted in Figure 2, the models with the most evidence of positive impact included some or all elements of care management.
Interdisciplinary primary care models demonstrated the greatest number of positive impacts. This includes quality of life, quality of care, patient satisfaction, utilization, and overall cost of care.
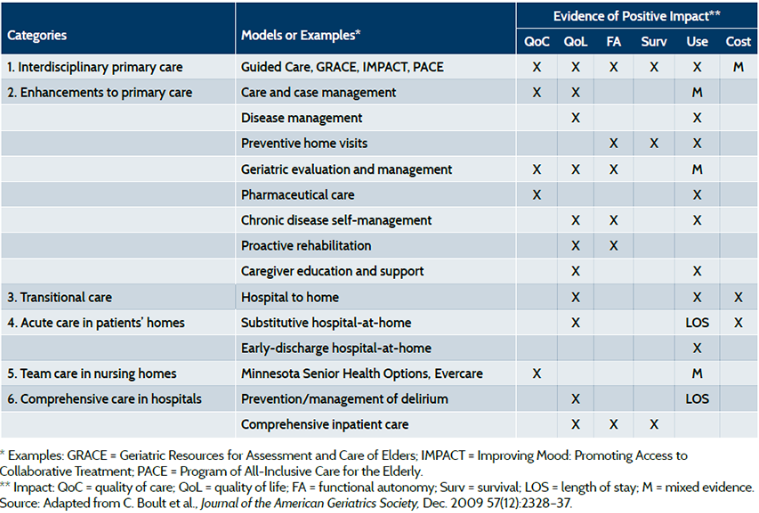
Figure 2: Care models with evidence of positive impact. Source.
This research identified several characteristics of care management programs that tended to meet both patient and provider objectives.
The most successful programs had seven common aspects, including:
- Identifying and enrolling patients with complex needs, however, not so severe that palliative or hospice care would be more appropriate
- Using specially trained care managers on multidisciplinary teams that include physicians
- Supplementing telephone calls to patients with frequent in-person meetings and occasional in-person meetings with providers
- Providing educational support to patients
- Coaching patients and families to engage in self-care, including helping patients manage medications
- Recognizing problems early and intervening quickly to avoid emergency visits and hospitalizations
- Partnering with informal caregivers in the home to support patients toward their goals
Other research examined 18 primary care-integrated complex care management programs. It identified common managerial and operational approaches that achieved the best outcomes, including:
- Focusing on building trusting relationships with patients and their primary care providers
- Matching team composition and interventions to patient needs
- Offering specialized training for team members
- Using technology to bolster care management efforts
Once care teams clearly understand their goals, the distinct objectives patients have, and evidence-based best practices, they need one last piece to put it all together.
ThoroughCare helps care teams and patients meet their respective care management objectives
ThoroughCare is an end-to-end care management solution that provides everything providers need to deliver patient-centered engagement. ThoroughCare ensures providers meet their care and financial objectives, including:
- Identifying the most appropriate patients
- Seamless program enrollment
- Standardized care management workflows
- Robust analytics and reporting
- Automated time tracking and CPT billing
