
.jpg "Daniel Godla")
Physicians and other qualified providers working within nursing and assisted living facilities can deliver covered care management services, according to The Centers for Medicare & Medicaid Services (CMS). So long as they meet all billing requirements, and the claim is submitted using a specific NPI number. These services include:
- Behavioral Health Integration (BHI)
- Chronic Care Management (CCM)
- Principal Care Management (PCM)
- Remote Patient Monitoring (RPM)
- Transitional Care Management (TCM)
Nursing homes can use these programs, in alignment with a data-driven, team-based approach, to improve chronic disease management, enhance patient satisfaction, and drive additional revenue.
Nursing home trends align with care management value
Post-acute and long-term care organizations are facing workforce shortages and increased staffing requirements. Nursing organizations are seeking new ways to support residents and create new revenue streams due to several trends, including:
Value-based care: Nursing homes, particularly skilled nursing, are more frequently creating or contracting with insurers through value-based care (VBC) arrangements. VBC partnerships that include post-acute care nursing emphasize chronic disease management, quality performance to reduce hospital readmissions, and improving patient outcomes.
Care coordination: Because of their unique position in the healthcare ecosystem, nursing homes are fostering tighter partnerships and collaborative services with healthcare providers, payors, and other stakeholders. They’re playing a more significant role in providing comprehensive and integrated care, including care transitions. This enhances their value among primary care physicians, specialists, and pharmacists.
Preventive care: Nursing homes can proactively address health issues that cause readmissions and chronic illness exacerbations. Increasingly, nursing facilities are incorporating preventive measures that have an outset impact on senior health, including fall prevention programs and chronic disease management.
Personalized care: Healthcare organizations are using population health, analytics, and team-based care to provide more tailored interventions. These are based on an individual’s needs and health goals.
Patient and family satisfaction: Current and future payment models place greater emphasis on patient and family satisfaction. Through more collaborative communication and coordination, nursing homes can improve satisfaction scores, impact shared savings in VBC, and attain higher quality ratings.
Data-driven decision-making: More nursing homes, particularly skilled nursing facilities (SNFs), collect data on patients with two or more chronic diseases. They do so to design holistic care plans via evidence-based predictive analytics. In addition to preventing escalating medical risk, tapping clinical, performance, and operational data allows leaders to assess the strategic value of different programs and interventions. This is the heart of success in a managed or value-based care model.
Care management supports value-based contracts
Chronic Care Management (CCM) can be implemented as a Medicare fee-for-service program or be integrated within a VBC contract. No matter the payment arrangement, CCM helps patients avoid high-risk, costly outcomes, such as frequent emergency department visits, hospital readmissions, and higher mortality rates.
A study published in 2023 found that standardized care management protocols implemented in a skilled nursing facility could reduce readmission rates by nearly 50% (from 23.5% to 12.1%). This was particularly true for patients with COPD. Protocols similar to those used in care management included clinical assessments, multidisciplinary care planning, and medication management.
Institutional Special Needs Plans (I-SNPs)
One VBC model allows long-term care providers to lead special needs health plans.
A growing number of long-term care providers, nursing facilities, and assisted living companies are forming their own SNPs.
With over 100K enrollees, SNPs limit their geographic market area, allowing benefit flexibility, including primary care services and care management. These VBC characteristics enable long-term care providers to take on more risk for quality and cost outcomes for higher-acuity adults.
From 2015-2020, 33% of all SNPs were led by long-term care organizations.
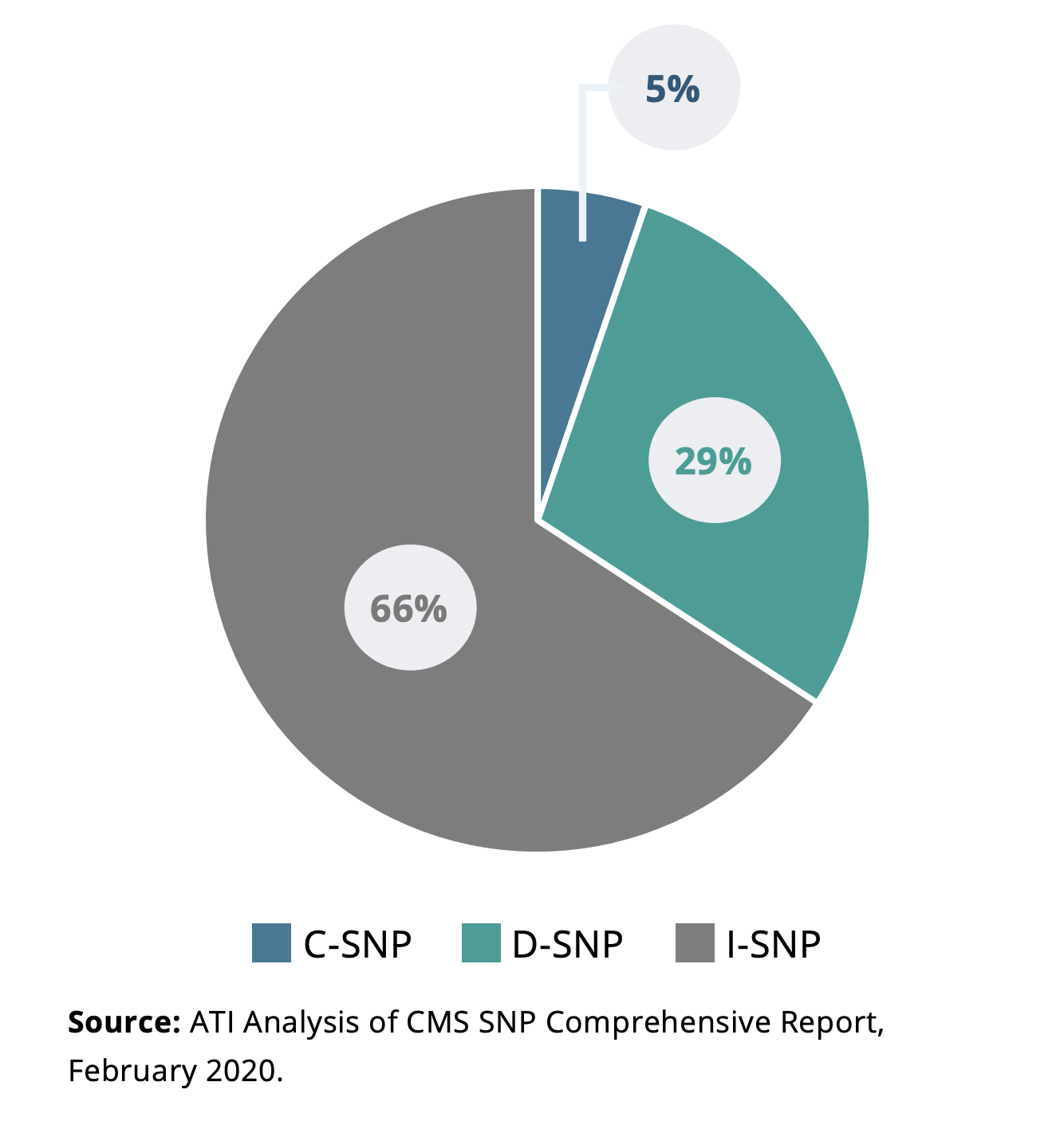
One type of SNP—Institutional Special Needs Plans (I-SNPs)— restricts enrollment to Medicare Advantage beneficiaries who have had or are expected to need a higher level of nursing services for 90 days or more.
In 2020, 66% of SNPs were I-SNPs, as indicated in Figure 1.
A 2020 case study analysis highlights the value long-term care provider-led SNPs offer vulnerable and medically complex beneficiaries. This research revealed six competencies necessary to achieve care, quality, and financial objectives, as shown in Figure 2.
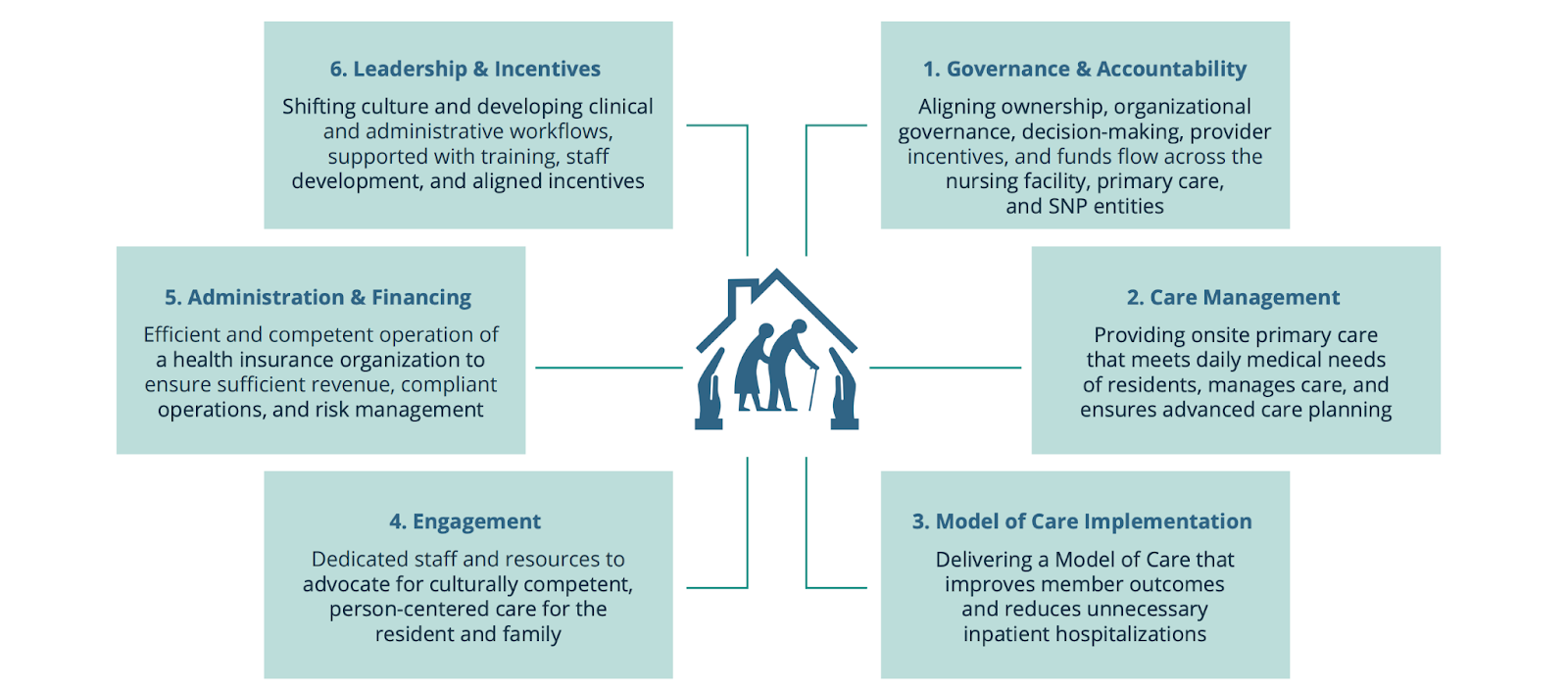
Figure 2: Case study-informed research reveals six critical requirements for LTC SNP success. Source.
Accountable Care Organizations (ACOs)
Nursing care organizations, including skilled nursing facilities, are launching or partnering with accountable care organizations (ACOs). Currently, more than 2,300 ACO-SNF affiliates participate in the Medicare Shared Savings Program as next generation ACOs.
A traditional ACO seeks to generate savings by reducing stays in a nursing home or eliminating SNFs altogether. Multiple studies have confirmed that ACOs can be effective in this goal.
Nursing homes use the ACO model to provide additional value from their vantage point in the care continuum. Physician groups are developing VBC models and partnerships with long-term care facilities as a population often overlooked by current value-based programs.
Their main objectives are to reduce the multifactorial risks for readmission and minimize the disruptions to residents’ quality of life.
ThoroughCare enables end-to-end care management
ThoroughCare is an end-to-end solution for Chronic Care Management and other programs, such as Transitional Care Management and Remote Patient Monitoring. For nursing homes, ThoroughCare gives care teams everything they need to streamline patient enrollment and engagement, develop comprehensive, personalized care plans, and track and report billable services.
