

Screening for health-related social needs (HRSN) is evolving into a care standard.
Value-based care contracts and accreditation bodies are beginning to require screening for social determinants of health (SDOH) and social needs.
The Joint Commission now asks healthcare organizations to assess HRSNs for a representative sample of their patients. Their focus on health-related social needs highlights the needs of individuals versus social determinants of health that describe population characteristics and influences.
Health systems, ambulatory settings, and health plans will begin to see more screening requirements for HRSN or SDOH. However, most will leave the choice of which tool or questions to use up to the healthcare organization.
While there has been little research into health-related social needs or SDoH assessment tools, several have been validated and reviewed. These options are in alignment with the Institute of Medicine's (IOM) recommendations and other healthcare quality organizations' requirements.
Setting the stage for health-related social needs and SDOH screening
Despite a proven link between SDOH and health outcomes, a 2020 Population Health Management research review estimated that 50% of patients with social needs could be missed by failure to screen routinely.
According to the National Academies of Sciences, social needs should be screened into five main categories, including:
- Race, ethnicity, and cultural circumstances
- Socioeconomic
- Gender
- Social relationships
- Residential and community environment
In 2014, the IOM convened a committee to identify which social and behavioral domains most strongly correlated with health. The committee recommended 11 candidate SDoH data domains, including education, financial resources, race/ethnicity, social support, violence, and neighborhood.
More recently, CMS suggested prioritizing screening for SDOH domains that can be addressed through community services, including:
- Housing instability
- Food insecurity
- Transportation access
- Utility assistance
- Interpersonal safety
Equipped with appropriate screening tools, clinical and non-clinical staff can uncover a patient’s health-related social needs and use that information to create effective care management plans.
Choosing among validated social needs and SDOH assessment tools
The following social needs assessment tools are among those provided as resources by the Joint Commission, along with many other screening support materials and education.
- The Health-Related Social Needs (HRSN) Screening Tool includes 10 items categorized into five domains: housing instability, food insecurity, transportation problems, utility help needs, and interpersonal safety. This tool leverages other validated assessments.
- The Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences (PRAPARE) is a nationally standardized patient risk assessment protocol based on national core measures.
- Developed by a nonprofit organization founded by physicians and public health innovators, the HealthBegins screening tool assesses 12 domains and provides a minimum frequency for re-assessment.
- The American Academy of Family Physicians (AAFP) created an SDOH short form that includes 11 questions on housing, food, transportation, utilities, personal safety, and the level of assistance needed.
- AccessHealth created a social determinants screening tool as a companion to the Center for Health Care Strategies’ brief, Screening for Social Determinants of Health in Populations with Complex Needs: Implementation Considerations.
- CMS created the Accountable Health Communities Health-Related Social Needs Screening tool to assess needs in 5 core areas: housing instability, food insecurity, transportation problems, utility help needs, and interpersonal safety.
While some tools focus on a single social need area (i.e., food insecurity), others focus on multiple factors.
Ensuring HRSN and SDOH screening tools fit organizational objectives
When vetting and implementing a screening tool, healthcare leaders should tailor it to meet the unique needs of their SDOH or care management program, patient population, and programmatic goals.
Consider these steps when adapting or adopting a screening tool:
- Confirm that questions are written at an accessible reading level for your patient population
- Pilot your chosen tool before committing to it or scaling its use to more programs or populations
- Consider the published research on individual instruments and vet those tools with your clinical and program leaders
- Ensure that the new tool doesn’t overlap with existing surveys or EMR questions to avoid redundant data collection
- Integrate your chosen social needs screening tool into existing clinical and care management workflows
- Capture screening data in digital form through your EMR or care management platform
Support care management and SDOH interventions with health-related social needs screening data
Once you’ve vetted and selected your HRSN screening tool, implement a regular review of SDOH data output. Look at how its collection is connected to addressing social needs and improving health outcomes.
When social needs data input and output align well with available community resources, care management programs can make a measurable impact on patient health and support quality and payment incentives.
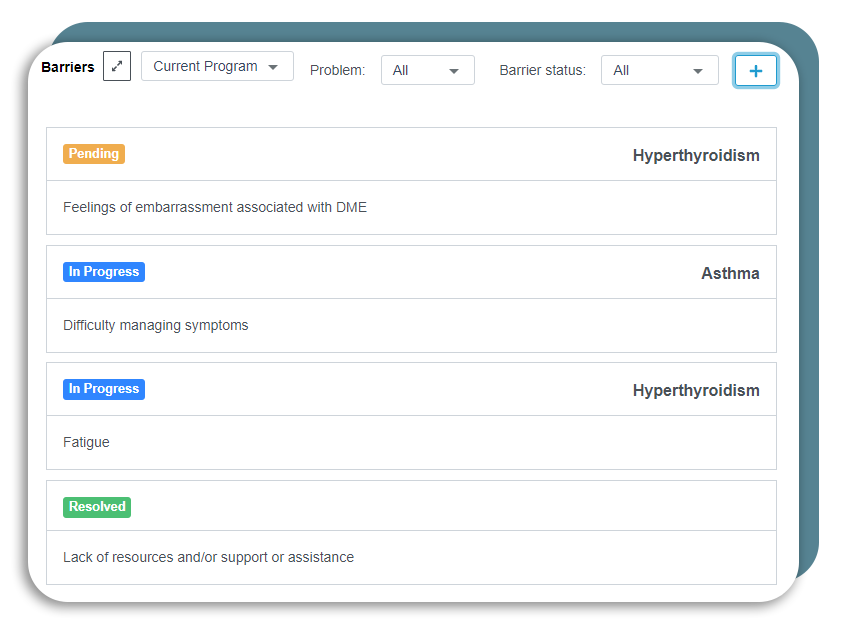
ThoroughCare can help assess social barriers as part of patient–centered care planning.
How ThoroughCare can help
Healthcare organizations use ThoroughCare to deliver integrated care management services to foster patient engagement and enhance revenue. Our platform provides the digital infrastructure to leverage fee-for-service programs for value-based success.
With seamless EHR integration and data interoperability across health information exchanges and remote devices, our platform supports solutions for:
- Chronic disease management
- Remote patient monitoring
- Behavioral health services
- Wellness assessments
- Transitional care
Providers use ThoroughCare to seamlessly manage populations, capture and act on patient data with interactive care planning and assessments, and visualize business performance to inform decision-makers.
